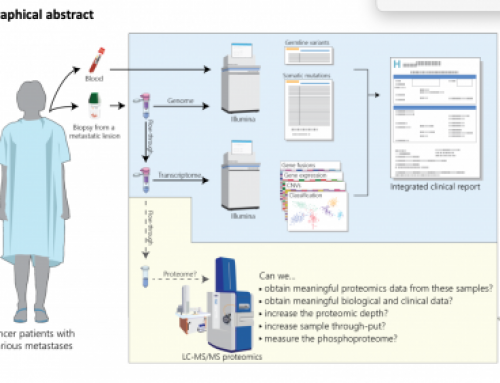
A recent paper in Nature Scientific Reports from Maurice Jansen’s group at the Erasmus Medical Centre in Rotterdam presents ctDNA analysis by targeted NGS from just 250pg of input cfDNA . This is a very small amount of material, and although the authors do discuss the impact of false-negatives with such low volumes of serum cfDNA, they do report very good results.
The team sequenced a 45-gene panel on the Ion PGM system for ten metastatic breast cancer patients in their primary tumour DNA (using standard DNA quantities) and 3 consecutive serum samples (using the 250pg protocol).

Weerts 2017 Fig 4
How much ctDNA
Many ctDNA studies use 1-5ng of input ctDNA but the Erasmus team used only 265-445 pg. This is half, to 10-fold lower amounts of ctDNA than would normally be reported. Their results suggest that even these minute amounts of ctDNA can generate comparable data to standard protocols. However they did report a few of the samples processed from minute quantities of material had unexpectedly high numbers of variants – possibly due to an accumulation of PCR errors, amplification bias or variability in length of DNA fragments.
In their discussion they talk about the limitations of using minute quantities of ctDNA, primarily the limit of detection (2% variant frequency) since 250 pg input represents approximately 36 diploid cells thus allowing the detection of 1 mutant copy in 72 wildtype copies. This has to be balanced against the need to detect lower frequency alleles which can be detected at well under 1% using larger amounts of samples, and different technologies (although the group make no arguments about the choice of technology affecting on sensitivity, putting this all down to the amount of sample used).
How to collect cfDNA
The paper also references earlier work by Dennis Lo’s group in 2016 on the impact of collection tube on the yield and quality of cfDNA. This was published in 2016 but anyone working on cfDNA should be thinking very carefully about their collection protocols as blood that is handled badly will result in very high contamination from gDNA. Potentially making the sample useless for ctDNA (or foetal cfDNA) analysis.
Key to their experiment were very tight protocols on sample collection. All samples were collected simultaneously (that’s a lot of needles at once) into Vacutainer® plastic EDTA, Sarstedt Serum Z, and either one of the following sets of tubes: Greiner Bio-One Vacuette® Z Serum Separator Clot Activator or Greiner Bio-One Vacuette® Z Serum Clot Activator. Blood was held at room temperature for 2 hours, blood samples were centrifuged at 1600 g for 10 min at 4 °C. Then plasma and serum fractions were re-centrifuged at 16,000 g for 10 min at 4 °C, and stored at − 80 °C.
They showed that the percentage contributions of different tissues varied between collection method by methylation analysis (Fig 5). With the most DNA coming from the placenta in the plasma samples. This is likely to be important for ctDNA collection as well, as the type of collection will affect the proportion of tumour derived DNA in the sample.

Lo 2106 Fig 5
The paper also states that “cfDNA concentration in serum is a summation of two opposing processes: DNA degradation or removal, and contamination of genomic DNA from white blood cells”. They suggest that serum should not be used because of contamination by genomic DNA from leukocytes; and because of degradation during collection. Unfortunately this was a tiny study with just 13 subjects analysed.
PS: One thing missing from the Lo group paper was the use of Streck tubes. These are currently the (expensive) gold standard and I’d be interested in more up-to-date comparisons if you know of any!







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I think they sequence background noise. I would not consider this method for clinical applications… What do you think of the [DNA]input…
I don’t think this is just noise they are reporting, but there will be huge issues with sensitivity. There are likely to be so few molecules present that important mutations may be missed – however the authors do address this. I think more is required to understand where we lose moelcules in ctDNA library prep, currently most of the ctDNA is not assayed in the final library. Improving this would lead to big gains in sensitivity and make this kind of low conc DNA analysis much easier to believe.